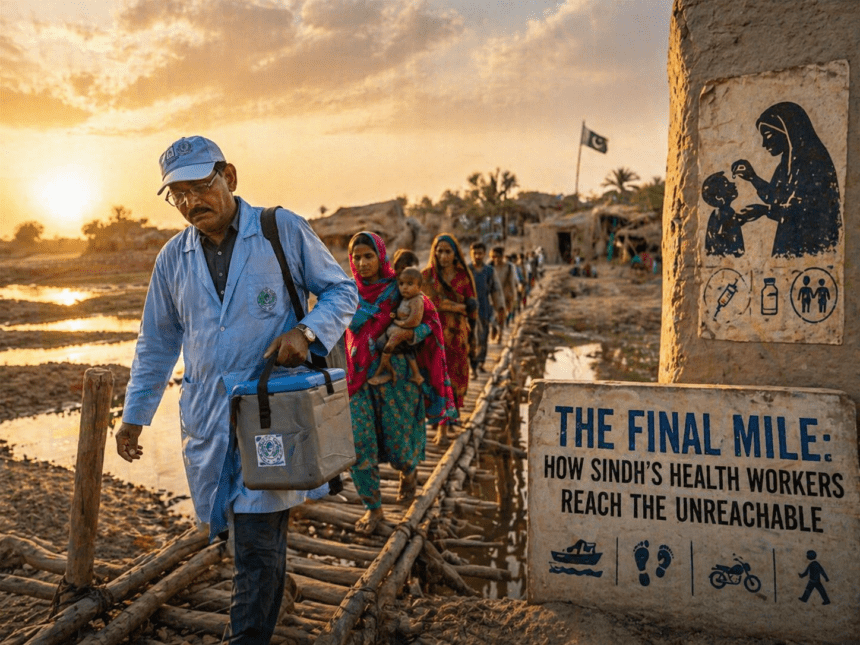
In the sweltering heat of Sindh’s remote riverine belts, the path to a polio-free Pakistan often ends where the paved road stops. For vaccinator Asif Ali, the mission isn’t just about medicine; it’s about navigating shifting sandbanks and distrust in communities that have seen little of the state.
He carries a chilled carrier containing oral polio vaccine (OPV) drops. Behind him, a local police guard keeps a watchful eye.
This is the “final mile”—the most dangerous and difficult stretch of the global effort to eradicate a virus that remains endemic only in Pakistan and Afghanistan. The logistics are brutal. In districts like Dadu or Ghotki, health teams often swap motorcycles for wooden boats to reach families living on islands in the Indus River.
These aren’t just logistical hurdles; they are constant barriers to consistency. If a child misses a single round of drops, the immunity gap widens. “People ask why we keep coming back,” Ali said, wiping dust from his face after a four-hour trek. “They don’t see the virus, so they don’t fear it. They fear the lack of clean water and basic food more. We have to earn their trust before we can even open the vial.”
The skepticism isn’t entirely misplaced. Decades of sporadic health interventions have left a vacuum of credibility in rural Sindh. When a team arrives, parents often weigh the promise of protection against the reality of their daily struggle. The health department has attempted to bridge this by hiring local women—community health workers who speak the dialect and know the family dynamics—but the turnover remains high due to meager, delayed stipends.
Data from the Regional Polio Laboratory shows a persistent struggle in keeping environmental samples clear of the virus. Even when vaccination coverage hits 90% in urban centers, the “invisible” pockets in Sindh’s interior act as reservoirs.
A single case in a remote village can trigger a resurgence in a major city like Karachi within weeks, carried by the constant flow of migrant labor. The strategy is shifting. Instead of mass, high-speed campaigns that often miss mobile populations, the government is moving toward “micro-planning.
” This involves mapping every household in the riverine areas and stationing permanent transit teams at bus terminals and boat crossings. It’s slower, more expensive, and requires far more patience than a standard drive.
Yet, for the teams on the ground, the math is simple. If they stop, the virus spreads. If they keep moving—through the mud, the heat, and the social barriers—the window for the disease keeps closing. As the sun sets over the Indus, Ali packs his empty carrier.
There are no cameras here, no press releases, and no fanfare. Just another village covered, another handful of children protected, and a long walk back to the road before dark.