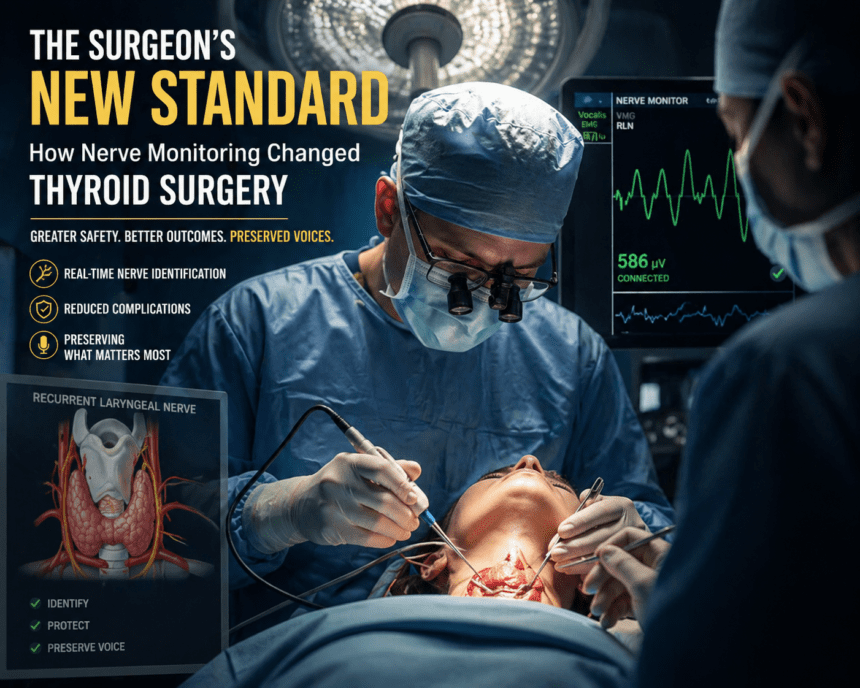
The Surgeon’s New Standard: How Nerve Monitoring Changed Thyroid Surgery Thyroid surgery once carried a distinct, terrifying risk: the permanent loss of a patient’s voice. Surgeons relied on visual identification to avoid the recurrent laryngeal nerve—a thin, critical wire responsible for vocal cord movement. If that nerve was nicked or stretched, the patient risked everything from a raspy whisper to permanent airway obstruction.
That margin for error is shrinking, thanks to Intraoperative Nerve Monitoring (IONM). The technology functions like a specialized GPS for the surgeon.
By placing an endotracheal tube equipped with surface electrodes between the patient’s vocal cords, the surgical team can monitor nerve activity in real-time. If the surgeon’s instrument gets too close to the nerve, an alarm sounds. It provides an objective, audible warning long before damage occurs.
“The visual approach was never enough,” said Dr. Elena Rossi, a head and neck surgeon who has integrated monitoring into her practice for the last five years. “You’re working in a crowded, bloody field. Nerve monitoring gives us a second set of eyes where we can’t actually see.
” The shift is statistical, not just anecdotal. Data from the International Neural Monitoring Study Group shows that surgeons using IONM report significantly lower rates of temporary vocal cord paralysis compared to those relying on sight alone. For patients, this means the difference between a routine recovery and weeks of intensive speech therapy.
Despite the benefits, the technology isn’t a silver bullet. Critics point out that it creates a false sense of security for inexperienced surgeons. Relying on a machine can lead to complacency, potentially causing a surgeon to skip the foundational anatomical training that still defines surgical excellence.
“The machine tells you when you’re close, but it doesn’t do the surgery for you,” noted Dr. David Chen, a surgical educator. “It’s a tool for verification, not a replacement for knowing the anatomy by heart.” Insurance coverage remains a hurdle.
While most major carriers now recognize IONM as the standard of care for high-risk thyroidectomies, patients often face out-of-pocket costs for the specialized equipment used during the procedure. It creates a tiered system where the safest technology is sometimes reserved for those who can afford the premium.
As the industry moves toward wider adoption, the focus is shifting from “if” the technology should be used to “how.” Surgeons are now standardizing protocols, ensuring that the technology acts as a safety net rather than a crutch. For the patient, the conversation has changed.
A decade ago, the risk of voice loss was an accepted gamble. Today, it’s a variable that can be managed, monitored, and—in most cases—avoided entirely.