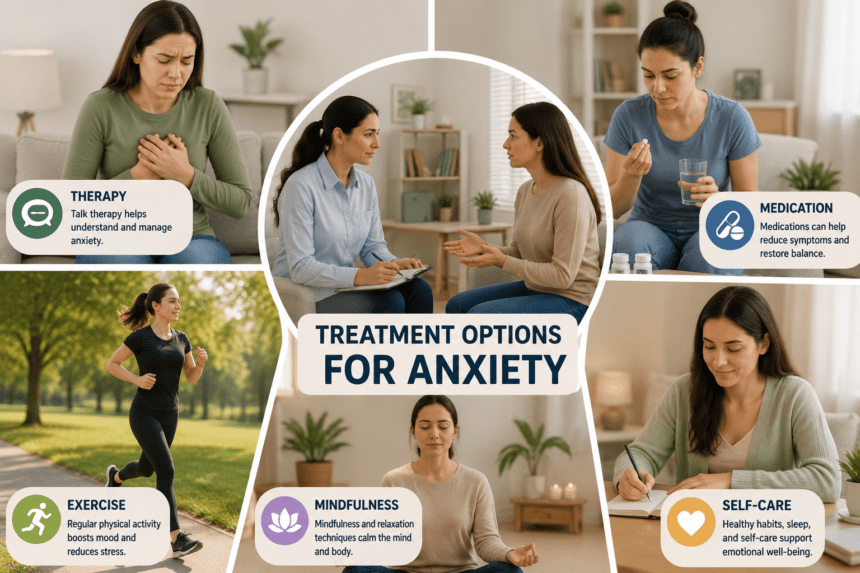
Prescription pads are no longer the default response to chronic anxiety. As clinical understanding of the nervous system shifts, psychiatrists and therapists are increasingly prioritizing behavioral interventions and lifestyle modifications over immediate pharmaceutical reliance.
The shift stems from a growing body of clinical data suggesting that while SSRIs and benzodiazepines provide symptomatic relief, they often fail to address the root physiological dysregulation.
For many patients, the “chemical imbalance” narrative is being replaced by a focus on nervous system conditioning. Cognitive Behavioral Therapy (CBT) remains the gold standard, but it’s evolving. Modern practitioners are layering “somatic experiencing” into traditional sessions. Instead of just talking through stressors, patients are trained to track physical sensations tight chests, shallow breaths, racing pulses in real-time.
By slowing down the body’s fight-or-flight response, patients learn to de-escalate their own biology without a pill.
Exercise, once dismissed as a “wellness” tip, is now being prescribed with clinical precision. High-intensity interval training (HIIT) and resistance training act as a controlled stressor, teaching the brain to recover from elevated heart rates. It’s essentially a gym session for emotional resilience. Dietary intervention is also moving from the fringe to the clinic.
New research into the gut-brain axis shows that chronic inflammation, often fueled by processed diets, exacerbates anxiety markers. Psychiatrists are now looking at blood panels for vitamin D, B12, and magnesium deficiencies before writing a single prescription.
Correcting these metabolic gaps often yields results that mirror mild anti-anxiety medication. Digital tools are filling the gap between therapy sessions. Biofeedback devices wearable sensors that track heart rate variability (HRV) allow patients to see their anxiety in data form.
When a user sees their HRV plummet, they know it’s time for a box-breathing exercise. It turns an invisible internal crisis into a measurable metric that can be managed. Despite these advancements, the medical community warns against a “DIY” approach. Severe, treatment-resistant anxiety often requires a combination of medication and therapy to stabilize a patient enough to begin the hard work of behavioral change.
The goal isn’t necessarily to eliminate anxiety a natural human response but to stop it from becoming a debilitating lifestyle.
For the millions navigating this, the focus has moved from “fixing” a broken brain to training a reactive one.